Helping Get You Maximum Compensation Since 1955
The Concussion Return to Play Guide for High School Athletes
Contact Us Now
The Concussion Return to Play Guide for High School Athletes
Watch just one football game, and you will see each player endure numerous physical hits to the body and head. Studies are now concluding that many student athletes are suffering concussions in football and other sports in which physical contact occurs. Studies confirm that concussions are happening at a much higher rate than is reported because the physical, cognitive, and emotional effects often go undetected.
Parents, coaches, and doctors must understand how serious traumatic brain injuries are. Important factors include the proper diagnosis, whether and when athletes can resume playing sports, what symptoms to look for, and the short—and long-term effects of concussions. Some liability issues involved in sports injuries include who is responsible for the concussion and what precautions should have been taken to prevent or reduce the severity of the injury.
Communities must know the risks of excessive high school and college sports contact. Parents should be informed of their rights and remedies (and the rights of the student athlete) when a son or daughter suffers a traumatic brain injury, which can cause suffering, significant changes in functioning, or even death.
What is a concussion?
A concussion is a type of brain injury, usually caused by an impact or trauma. The brain, an organ that weighs about three pounds, floats inside the human skull, protected by cerebrospinal fluid.
An impact or trauma can cause the brain to move about the skull abnormally, causing the brain to make contact with one side of the skull, called the coup, and then the other side, called the contrecoup.
An unnatural impact can also cause the head to rotate too quickly, called a rotational concussion, which can strain or damage brain tissues. Any type of concussion can cause neurological harm.
A parent, coach, relative, or friend who suspects that a child athlete may have suffered a concussion should review:
-
- Whether the child athlete suffered a direct impact to the head.
-
- Whether there was an indirect body impact, which may have caused neurological damage.
-
- If the child athlete suffers from any physical problems, such as headaches or nausea.
-
- If the child suffers from any cognitive difficulties, such as memory loss or difficulty focusing or concentrating.
-
- If the child suffers from any emotional issues, such as depression, sadness, or being irritable.
-
- If the child has daily living troubles, such as difficulty sleeping, a poor appetite, or a state of lethargy.
Parents and coaches need to understand:
-
- That high school athletes who suffer a concussion often need more time to heal, may suffer more severe symptoms, and may suffer more neurological damage than college-age and professional athletes may.
-
- That over half of high school athletes have already suffered a concussion before they even begin their high school sports career, and that over one-third of college athletes suffered multiple concussions.
-
- That for athletes under 25, specialized treatment is required because the frontal lobes of their brains are not yet fully developed.
For more information about what concussions are, please see these frequently asked questions prepared by the Sports Concussion Institute.
How to spot signs of a concussion
Some of the signs doctors and others look for are:
Concussions can be difficult to diagnose. Sometimes the athlete loses consciousness, but there is usually no such loss.
-
- Physical symptoms
-
- Blurred vision
-
- Headaches
-
- Lack of balance
-
- Light-headedness or dizziness
-
- Nausea
-
- Seeing flashing lights
-
- Sensitivity to light or noise
-
- Unequal pupils
-
- Vomiting
-
- Physical symptoms
-
- Cognitive symptoms
-
- Confusion
-
- Difficulty paying attention or focusing
-
- Inability to concentrate, think straight, or to absorb new information
-
- Cognitive symptoms
-
- Emotional symptoms
-
- An unusual amount of crying
-
- Anxiety
-
- Depression
-
- Irritability
-
- Lack of interest in daily activities, such as eating and socializing
-
- Sadness
-
- Emotional symptoms
-
- Daily activity symptoms
-
- Inability to fall asleep
-
- Irregular sleep – too little or too much
-
- Daily activity symptoms
For more information about concussion symptoms, see this report prepared by Head Health Management System.
Concussion Return to Play Guidelines
A child who has—or may have—suffered a concussion should not be rushed back onto the playing field. Athletes who return to the game too early are more likely to suffer another concussion and may suffer another serious injury because of their impaired performance.
The school, parents, and community should have policies in place to prevent children from returning to sports competition until they are really ready to play after an injury.
The following concussion return to play protocol from the American Academy of Pediatrics (AAP) should be considered by coaches, staff, and the team or individual doctor:
-
- Determine the diagnosis. A diagnosis should only be made after a thorough medical examination, including a full battery of standard concussion tests. The diagnosis helps determine appropriate treatment options and the duration of the recovery period.
-
- Review the relationship between the condition and athletic performance. In addition to cognitive abilities, the athlete’s physical endurance, strength, and coordination should be considered.
-
- Examine the risk factors and likelihood of a secondary injury. A combination of injuries can increase the likelihood of harm exponentially. Risk factors include the type of sport, the player’s position, and whether or not the child is playing a team sport, which poses greater risk for a collision.
-
- Review the treatments and symptoms. If the athlete is still suffering symptoms, he or she should not return to play. Players should not return prior to the standard healing time their doctor recommends or before treatment is complete.
-
- Explore safety issues. Safety can include the use of equipment such as helmets. It can also involve assigning the athlete a less strenuous position and one where there is less likelihood of physical contact. Practice hours can be limited, and other safety measures can be taken depending on the sport being played.
-
- Determine the medical guidelines that apply for concussions for the school, the league, and the medical community. Guidelines should be met before the player returns to competition.
-
- Get informed consent. High school competition generally requires the consent of the parent. Informed consent means fully advising the athlete (and the minor’s parents) about all the risks of continued play.
-
- Find out what the child athlete wants. Athletes, especially minors, may have legitimate fears about playing again. The child should not be pressured to participate in sports again before he or she is ready, if at all.
According to the Sports Concussion Institute study above:
-
- Risk factors also include the number and extent of prior concussions. Athletes who have had three concussions, for example, are three to nine times more likely to suffer a fourth concussion.
-
- There are some studies, again according to the CDC, that suggest that women are more likely to suffer a concussion, need more recovery time, and have more severe symptoms than male athletes.
-
- Other risk factors include a history of migraines or headaches and a history of developmental or psychiatric disorders.
Cognitive testing for sports injuries
According to the Nebraska Sports Concussion Network, doctors now use a variety of neurocognitive tests to help determine if a child athlete has suffered a concussion. These tests are conducted in addition to imaging tests like CT scans, MRIs, and PET scans. The imaging tests help to show structural brain abnormalities and are often done at the local emergency room. The imaging tests can show internal bleeding, lesions, and fractures. Still, these tests do not show the full picture.
Neurocognitive testing can show the ability or inability of the student athlete to reason, think, react, and focus. Parents and doctors should consider the following neurocognitive tests:
-
- Paper and pencil tests
-
- Sport Concussion Assessment Tool
-
- Paper and pencil tests
-
- Online computerized tests
-
- Immediate Post-Concussion Assessment and Cognitive Testing. The University of Pittsburgh Medical Center test evaluates attention, memory, brain processing speed, and other cognitive abilities. Many NCAA Division 1 football programs use this test, as do 75% of all Nebraska high schools.
-
- ANAM. Automated Neuropsychological Assessment Metrics
-
- CogState. Testing done by COGSTATE, a scientific cognitive testing company
-
- Online computerized tests
-
- Baseline Testing. These are tests conducted in the offseason to provide a preinjury view of the student’s brain functions.
-
- Post-Injury Testing. When a concussion is sustained or suspected, the baseline is given to the student again. Trained professionals then compare the baseline and post-injury tests for changes and abnormalities. The results help to determine if and when the student should play again and what other tests and treatments may be needed, including sending the injured athlete to a neurologist, neuropsychologist, or neurosurgeon. The post-injury test should be given after the athlete is symptom-free.
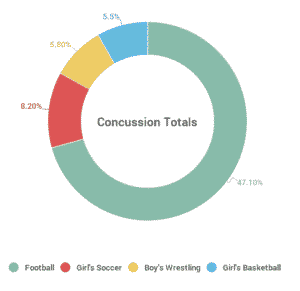
Concussions rates by sport among United States high school athletes
A study by the Center for Injury Research and Policy recently examined concussions suffered by high school athletes in the United States in 20 sports during the 2008 to 2010 school years. During that time, an estimated 300,000 sports-related concussions happened each year. The only activity, the report said, that causes more concussions among high school students is motor vehicle accidents.
Concussion Rates by Sport
The study found the following sports concussion statistics:
-
- The injury rate was six times higher for competition and games than for practice.
-
- The highest concussion totals per sport were as follows (from high to low):
-
- 47.1%
-
- Girls’ soccer. 8.2%
-
- Boys’ wrestling. 5.8%
-
- Girls’ basketball. 5.5%
-
- The highest concussion totals per sport were as follows (from high to low):
-
- 6.4%
-
- Boys’ ice hockey 5.4%
-
- Boys’ lacrosse 4.0%

-
- Common reasons for concussions were mostly player-to-player contact, followed by player-to-surface contact.
-
- Over half of the athletes returned to play in one to three weeks. Only 2% returned the same day.
Understanding the type of sport played, the type of contact, the gender of the players, and the risk factors involved can help implement safety and prevention measures aimed at reducing the risk of high school concussion injuries.
What are the symptoms of mild traumatic brain injury?
A concussion is a form of traumatic brain injury (TBI). A concussion is considered minor if the athlete loses consciousness or any confusion lasts less than 30 minutes. Even though diagnostic tests may be standard, the athlete may suffer physical, cognitive, or emotional problems. A mild TBI can do more than render the athlete unable to return to play. It directly affects the well-being of the player and those who live with the athlete.
According to Traumaticbraininjury.com:
-
- Concussions are also called minor head trauma, minor brain injury, minor head injury, or minor TBI.
-
- A mild TBI is often not properly diagnosed at the time of the injury.
-
- Even though the word mild is used, the injury can be quite serious. About 15% of people with a mild TBI diagnosis have symptoms that last for more than 12 months.
Symptoms after the injury are called “post-concussive syndrome.” Many of the physical, cognitive, emotional, and daily living symptoms have been described above (see the concussion symptom section). Additional symptoms can include loss of smell, changes in mood, light sensitivity, and audio sensitivity.
Symptoms can often be missed, in part, because they may not appear until days or even weeks after the initial trauma. It is important for family and friends to monitor the athlete. Family and friends are much more likely to notice the symptoms than the child athlete.
What are the symptoms of severe traumatic brain injury?
Athletes who suffer a severe traumatic brain injury often die or suffer permanent disability. According to the CDC, TBIs are a factor in almost a third of US injury-related deaths. Many other serious TBIs require the patient to be hospitalized. A severe TBI impacts more than just the victim. The family suffers as well.
Doctors, family, and coaches should understand how a TBI is classified. A common clinical tool is the Glasgow Coma Scale, which analyzes whether the patient is in a coma or is experiencing impaired consciousness.
The scale is:
-
- Severe TBI. 3 to 8
-
- Moderate TBI. 9 to 12
-
- Mild TBI. 13 to 15
Other scales used to review a TBI are:
-
- Abbreviated Injury Scale (AIS)
-
- Trauma Score
-
- Abbreviated Trauma Score
About 43% of patients with a severe TBI have a disability one year after the injury. Over five million Americans live with some TBI-related disability that limits their ability to function.
Sports injury case studies and their impact on your child
Several studies have been conducted on the effects of sports injuries. One prominent study at the Florida Center for Headache and Sports Neurology scanned the brains of 40 former National Football League (NFL) players who had recently retired from the game. The study found that 43% of these players averaged age 36 and had more white brain matter damage than healthy 36-year-olds. White matter is a vital brain factor for learning. White matter damage, another way of saying traumatic brain injury, can lead to chronic traumatic encephalopathy, Alzheimer’s, and other brain conditions.
The study did not find a direct link between the number of concussions a player suffered and the amount of white matter damage. There did appear to be a link between the number of physical hits and white matter damage. The NFL is now determining the right balance between protective research and recommended treatments, the safety of current and future NFL players, and the cost of settling legal claims by prior NFL players.
The NFL research may, in time, help high-school and college athletes. Still, more studies need to be done to determine the dangers to children and the best community and medical course of action in the treatment and prevention of TBI and other sports-related injuries among children.
Contact us today
The NJ traumatic brain injury lawyers at Aiello, Harris, Abate Law Group PC are experienced personal injury attorneys. They work with medical professionals, including neurologists, to help determine the cause of sports-related concussions, what steps could have been taken to prevent the injury, and the medical care needed to treat the condition.
Call us today at (908) 561-5577 or contact us. Your initial consultation will take place over the phone, and you can schedule an appointment at one of our office locations across New Jersey.
Contact our The Concussion Return to Play Guide for High School Athletes
Meet Our Team
The Aiello Harris Abate Law Group is made of a group of professionals that are here to help you through all challenges.
Get to Know UsLegal Practice Areas
Our law firm does not stop at The Concussion Return to Play Guide — take a look at how we can help you overcome your legal obstacles.
View all Practice Areas